| Tweet |

Custom Search
|
|
 
|
||
|
IMMERSION FOOT (TRENCH FOOT) Immersion foot, which may also occur in the hands, is a cold injury resulting from prolonged exposure to wet, cold temperatures just above freezing. It is often associated with limited motion of the extremities and water-soaked clothing. Remember that the temperature does not need to be below 32F (0C) to cause this injury. In the early stages, the feet and toes are pale and feel cold, numb, and stiff. Walking becomes difficult. When preventive action is not taken, the feet swell and become painful. In extreme cases, the flesh dies and amputation of a foot or of a leg maybe necessary. TREATMENT. In treating immersion feet (or hands), handle the injured parts very gently. They should not be rubbed or massaged. Get the victim off his feet as soon as possible. Remove wet shoes, socks, and gloves to improve circulation. Do not rupture blisters or apply salves or ointments. The feet may be cleansed carefully with soap and water, dried, elevated, and exposed to dry air. Keep the victim warm and transport him to a medical facility as soon as possible. Always evacuate immersion foot victims by litter. FROSTBITE Frostbite occurs when ice crystals form in the skin or deeper tissues after exposure to temperatures of 32F (0C) or lower. Depending upon temperature, altitude, and wind speed, the exposure time necessary to produce frostbite varies from a few minutes to several hours. The areas most commonly affected are the face and extremities. The symptoms of frostbite are progressive. Victims generally incur this injury without being acutely aware of it. Initially, the affected skin reddens, and there is an uncomfortable coldness. With continued heat loss, there is a numbness of the affected area because of reduced circulation. As ice crystals form, the frozen extremity appears white, yellow-white, or mottled blue-white, and it is cold, hard, and insensitive to touch or pressure. Frostbite is classified as superficial or deep, depending on the extent of tissue involvement. Superficial Frostbite In superficial frostbite, the surface of the skin feels hard, but the underlying tissue is soft, allowing it to move over bony ridges. This is evidence that only the skin and the region just below it are involved. TREATMENT. A minor case of superficial frostbite is fairly common and serves as a warning. Superficial frostbite can usually be thawed with body heat. Hands can be rewarmed by placing them under the armpit, against the abdomen, or between the thighs. Feet can be rewarmed by using armpit or abdomen of a buddy. Other areas of superficial frostbite can be rewarmed by warmwater immersion, skin to skin contact, or covered hot-water bottles. NEVER RUB a frostbitten area. Deep Frostbite In deep frostbite, the freezing reaches into the deep tissue layers. There are ice crystals in the entire thickness of the extremity. The skin does not move over the bony ridges and feels hard and solid. TREATMENT. The objectives of treatment are to protect the frozen area from further injury, to thaw the affected area rapidly, and to be prepared to respond to circulatory or respiratory difficulties. Carefully assess and treat other injuries first. Constantly monitor the pulse and breathing of the victim since respiratory and heart problems can develop rapidly. Be ready to administer CPR. Make no attempt to thaw the frostbitten area when there is a possibility of refreezing. Freeze-thaw-freeze will result in extension of the injury and may result in amputation. Treat all victims with injuries to feet or legs as litter cases. When this is not possible, it has been proven that walking does not lessen the chances of successful treatment as long as the limb has not been thawed out. When adequate protection from further cold exposure is available, prepare the victim for rewarming by removing all constricting items of clothing, such as gloves, boots, and socks. Boots and clothing frozen on the body should be thawed by immersing them in warm water before removal. Rapidly rewarm frozen areas by immersion in water at 100F to 105F (38C to 41C). Keep the water warm by adding fresh hot water, but do not pour it directly on the injured area. Ensure that the frozen area is completely surrounded by water; do not let it rest on the side or bottom of the tub. After rewarming has been completed, pat the area dry with a soft towel. Avoid pressure, rubbing, or constriction of the injured area Keep the skin dry with sterile dressings, and place cotton between the toes and fingers to avoid their sticking together. The general morale and comfort of the victim may improve by giving him hot, stimulating fluids, such as tea or coffee. Do not allow the victim to smoke or use
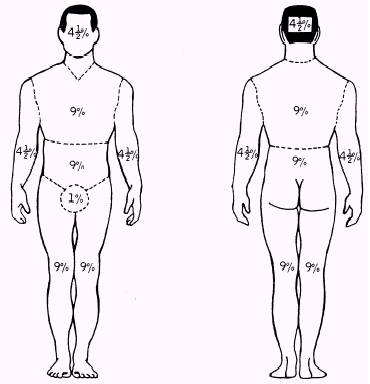
Figure 10-44.-Rule of nines. alcoholic beverages while he is being treated at the first-aid level. NEVER attempt to thaw frozen limbs by rubbing, exercising, or heating them in front of an open fire. Transport the victim to a medical facility as soon as possible. During transportation, slightly elevate the frostbitten area and keep the victim and the injured area warm. DO NOT ALLOW THE INJURED AREA TO BE EXPOSED TO THE COLD. |
||
|
||